 | |||
Pancreatic stone protein / regenerating protein | |||||
Pancreatic stone protein (PSP) was detected by the group of H. Sarles in the eighties of last century, based of observations made in the seventies. It was clearly characterized as a secretory protein present in as yet unclear physiological conditions. A few years later, a new protein was identified as part of the endocrine organ (islets of Langerhans), produced after the islets had been damaged. It was called regenerating protein (Reg). Its sequence turned out to be identical to PSP. Subsequently, the protein was referred to either names, depending on which part of the pancreas was worked on. Possibly the choice also reflected whether their was a true belief in the respective functions and anatomical localisation associated with the protein. Next to the initial PSP/Reg1, a second protein pancreatitis associated protein (PAP) was identified, clearly secreted in response to pancreatic damage. Depending on the species, several isoforms of PSP and PAP were detected. As PSP was named reg I, another protein was named reg 2, however, its identity and function was not unequivocally demonstrated. Thus, PAP was then named reg III to clearly define it as a new protein family. For a summary of the literature, use the following links: | |||||
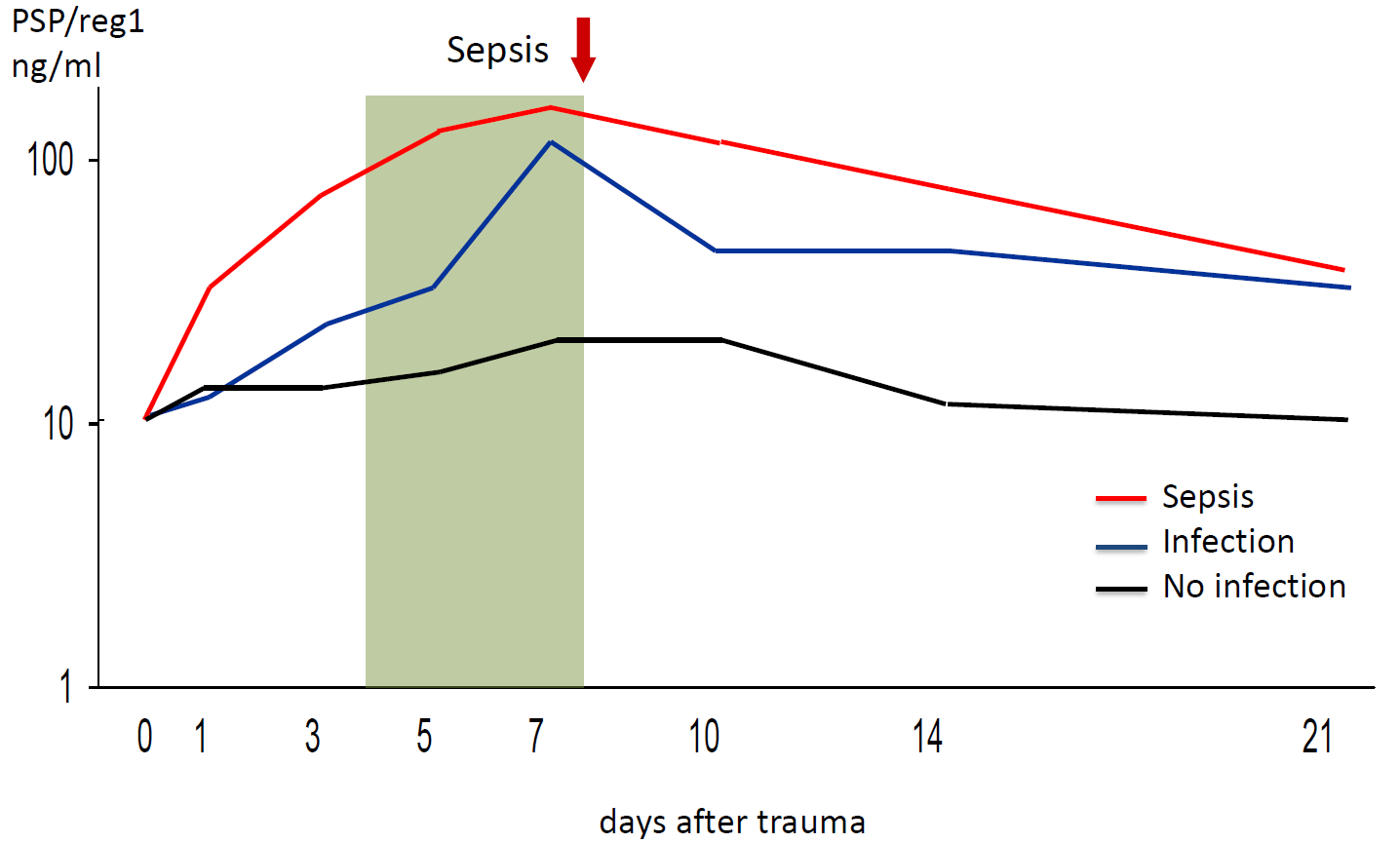 Development of PSP levels after a traumatic incident. Patients were grouped according to the clinical evaluation during the disease. 2-3 days before sepsis was diagnosed, PSP levels significantly increased, as depicted by the shading. Diagram simplified from Keel M. et al Critical Care Medicine 2009,37:1642-8 | |||||
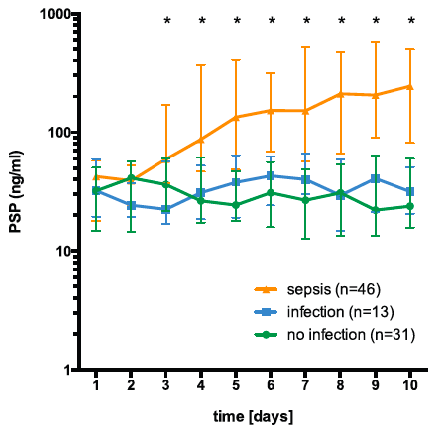 | Main effects analysis determined that PSP differentiated between infection, sepsis, and sterile inflammation from day 3 ongoing. PSP demonstrated a significant interaction between time and presence of sepsis wih a significantly steeper increase of PSP levels in septic patients as opposed to those exhibiting a nonseptic course (from Klein et al. Annals of Surgery 2020). | ||||
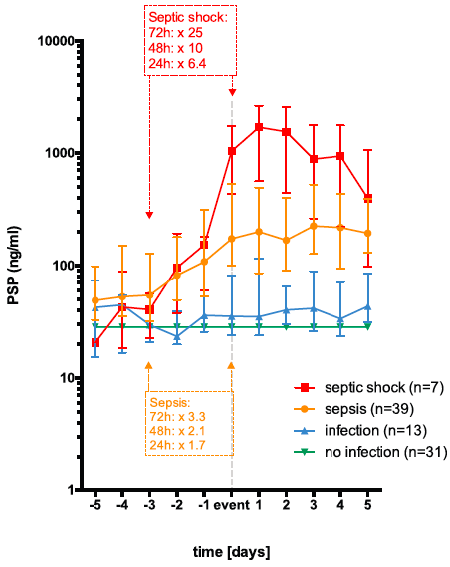 | Event-related depiction of PSP and routine inflammatory biomarkers. PSP serum levels tripled within 72 h and doubled within 48 h before a clinically apparent sepsis. In septic shock, PSP levels appeared 10-fold higher within 48 h before being clinically overt (from Klein et al. Annals of Surgery 2020). | ||||
©2018 The Pancreas Research Lab |